Below you will find information on some of the most common shoulder surgical procedures performed by Ms. Delaney. These are general guidelines, and each patient's individual case will be discussed in detail by Ms. Delaney prior to surgery.
In addition, you will find here the general pre-operative instructions that you should follow prior to any shoulder surgery with Ms. Delaney
General Pre-op Instructions
- Stop taking all non-steroidal anti-inflammatory medications (NSAIDs), for example aspirin (unless otherwise instructed by GP or cardiologist), ibuprofen (Neurofen), diclofenac (Difene), naproxen, celecoxib (Celebrex), mefenamic acid (Ponstan), etorocoxib, indomethacin etc. 7 DAYS prior to the date of your surgery.
- If you have been instructed by your GP or cardiologist to take daily aspirin, you must consult with him or her before you stop taking aspirin.
- If you are taking a blood thinner, for example warfarin, Plavix, rivaroxaban (Xarelto), dibagatran (Pradaxa), heparin or others, you MUST consult with the prescribing doctor for this medication on how to manage it around surgery and let our office know.
- HRT or the Oral Contraceptive Pill (OCP) should be stopped 6 WEEKS before the date of your surgery due to increased risk of blood clots in the veins of the legs or the lungs if these medications are continued through the surgical period.
- Stop taking all herbal supplements 10 DAYS before the date of your surgery.
- Do not eat or drink anything or have any chewing gum after MIDNIGHT the night before your surgery. If you are given an afternoon admission time, you may have tea and toast only, at 6AM on the morning of surgery, and then do not eat or drink anything after that.
- Shower the evening before or the morning of surgery with Hibiclens soap (a chlorhexidine antiseptic soap available at most pharmacies), and wash the affected shoulder area well.
- Remove all nail polish.
- Do not apply deodorant the morning of your surgery.
- If you are scheduled to have day-case surgery, you must be accompanied by a friend or adult relative to drive you home after discharge. It is not permitted for you to leave the facility unaccompanied after surgery.
- If you have any signs of infection, cough/cold, fever, skin irritation, dental infection etc., PLEASE call the office to let us know. It is better that we know in advance and address the issue with you before surgery rather than having to cancel your surgery last minute.
Nerve Blocks for Shoulder Surgery
Brachial Plexus Nerve Blocks for Shoulder Surgery
This leaflet has been prepared by Ms. Delaney in collaboration with Dr. Justin Lane, consultant anaesthetist and pain specialist, with input from patients who have had a nerve block for shoulder surgery and using material from the Royal College of Anaesthetists (UK) patient information leaflet.
Please pay particular attention to the information in the section After Surgery.
The brachial plexus is the network of nerve roots combining to form nerves that supply sensation and movement to the entire arm from shoulder to fingertips. A brachial plexus block is an injection of local anaesthetic around that group of nerves which temporarily blocks signals going through the nerves, including pain signals from the shoulder back to the brain. This can be helpful during and after shoulder surgery as it may lessen the amount of general anaesthetic drugs you need and therefore lessen the side effects of those, and it will also make the first night after surgery more comfortable. In certain cases, such as for capsular release for frozen shoulder, we use the window of complete pain relief provided by the block to start physiotherapy and get ahead of any potential for the shoulder to stiffen up again by having the physiotherapist stretch the shoulder immediately, while the block is keeping you comfortable.
Not all operations are suitable for nerve blocks and a nerve block may not be suitable for certain patients. The consultant anaesthetist taking care of you for your surgery will discuss the option of a nerve block with you if it is appropriate for your case and if the surgeon has requested it.
If you wish, you can be sedated when you have the nerve block injections or the nerve block can be performed after you are asleep under general anaesthesia. The anaesthetist will discuss with you which option is best for you.
We usually supplement the nerve block with a light general anaesthetic, because it can sometimes be difficult to sit still in the surgical position for the duration of your shoulder operation if you are awake with only the block providing regional anaesthesia.
The benefits of a brachial plexus nerve block include:
- Better pain relief after surgery
- Less need for strong pain killers, which can make you feel sick and may cause constipation or possibly have a risk of addiction if used for a long time
- Less need for a heavy dose general anaesthetic, which can lessen the side effects which include nausea/vomiting and prolonged drowsiness or tiredness
- Being able to get up and move around earlier after surgery and potentially leave hospital sooner
Before Surgery
You will have been given pre-operative instructions at the time of booking your surgery. It is important to note the instructions about fasting for a minimum of six hours before your procedure (to ensure an empty stomach and avoid the risk of food or liquid from your stomach coming up into your throat and lungs during your anaesthetic, which can be dangerous for you). It is also important that if you are taking any drugs to thin your blood that you let the surgeon and the pre-assessment team know which medication you are on so that a plan can be put in place as to whether you need to stop these drugs for a period of time before surgery or go on an alternative blood thinner temporarily around the time of your surgery. This may also need to be discussed with your GP and with any other prescribing doctor, for example a cardiologist if you have one, therefore it is important to let us know ahead of time.
Your anaesthetist will discuss the plan for your anaesthetic with you on the day of surgery and will explain the nerve block to you, if your case is appropriate for the option of a nerve block. You will have the opportunity to ask any questions at that time.
At the Time of Surgery
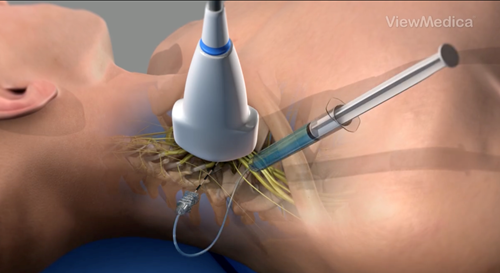
The nerve block will usually be done in a room near the operating theatre or it may be done in the operating theatre itself. The injection for a brachial plexus block is typically done in the side of your neck but additional injections may also be done close to your collar bone or shoulder blade or in your armpit. The skin is cleaned and some local anaesthetic is injected into the skin to numb it. The anaesthetist will then use either an ultrasound and/or a nerve stimulator which is a small machine that makes your arm muscles twitch to locate the nerves.
Most people find that the injection is no more painful than having an IV cannula placed or a blood sample taken. Your arm will start to feel warm and tingly and then heavy and numb. The injection can take 20 -40 minutes to start working, so in many cases you will go to sleep with your general anaesthetic before the arm is totally blocked and it is only when you wake up that you will experience the arm being numb and heavy. If you are given sedating medicine for the block or if the block is performed after you are first given the general anaesthetic drugs, you may not remember anything about receiving the nerve block injections.
After Surgery
If the block is working well, your entire arm from shoulder to fingertips will be “asleep” for the duration of the block, which can last up to 48 hours. Your arm will be numb and you will not be able to move any of the muscles. The sensation of not having any control over your arm and hand can be alarming but it is normal after the block and it is temporary. The nurses in the recovery room or on the ward may ask you to move your fingers in order to check whether your block is still in effect, this does not mean that they expect you to be able to move or feel, they are just checking to see if you are likely to need additional pain medication based on how well your block is working or not. You will need a sling to support the weight of your arm while the block is in effect.
While you cannot feel your arm and hand, take special care not to inadvertently injure yourself. Be particularly careful around heat sources such as fires or radiators or if using ice on your shoulder. You will not feel heat or cold while your block is working so pay attention not to burn yourself or cause cold injury to the skin.
Start taking your pain relief medication before the block wears off, as instructed. Do not wait until you feel pain to start taking pain relief as it can take time to then catch up and become comfortable. The block can sometimes wear off quite suddenly so it is important to get ahead of any potential pain.
When you start to feel some tingling or pins and needles and you start to regain some movement in your fingers, your block is starting to wear off and you should make sure that you have some pain relief on board as you will soon start to regain sensation in your shoulder after that.
If you are going to sleep for the night and you have still not regained sensation in the shoulder and therefore have no pain at all, which is very common the first night after surgery (and is a benefit as it helps you to get a good night’s sleep), make sure to take pain relief before going to sleep as it is possible that the block may wear off completely while you are asleep and if you have no pain relief on board, this may cause you to wake with pain that can be difficult to then control from a starting point of having no pain medicine in your system.
When to Seek Further Help
If you notice unexplained breathlessness or if your block has not fully worn off two days after the operation, you should contact your anaesthetist by calling the number given on your discharge paperwork.
Side Effects, Complications and Risks
Serious problems are uncommon but risk cannot be avoided completely. People vary in how they interpret words and numbers. This scale is provided to help.

Anaesthetists take a lot of care to avoid all the risks given in this section. Your anaesthetist will be able to give you more information about any of these risks and about the precautions taken to avoid them.
Risks:
- Injection in the side of the neck: hoarse voice, droopy eyelid, changes in your vision and possibly some shortness of breath. These side effects are common and temporary. They go away as the block wears off.
- Injection around the collar bone: there is a rare risk, less than 1 in 1,000, of damage to the covering of the lung (the pleura) which can lead to some degree of collapse of the lung – called a pneumothorax. Air goes into the space between the chest wall and the lung, called the pleural space. Treatment depends on how much air gets into this space – it may cause no symptoms at all or if it is a large amount and you become short of breath, you may need a chest drain (a plastic tube) to help manage it.
- All injection sites: it is common for a small blood vessel to be punctured, your anaesthetist will put pressure over the area to stop any bleeding.
- There is a rare risk of having a seizure or another life-threatening event. Your anaesthetist will manage any of these situations if they arise promptly and expertly.
- Nerve damage:
- The risk of long term nerve damage caused by a brachial plexus block leading to altered or loss of sensation or power is difficult to measure precisely. Studies show that it happens in between 1 in 700 and 1 in 5,000 blocks – meaning it is uncommon or rare.
- Very commonly, about 1 in 10 patients notices a prolonged patch of numbness or tingling in their arm. These symptoms will resolve within six weeks in 95% of these patients, and within a year in 99% of patients.
Biceps Tenodesis
Introduction
These are general guidelines, but each patient’s shoulder condition is unique and Ms. Delaney will discuss with you the specific details relevant to your case.
Biceps Tenodesis
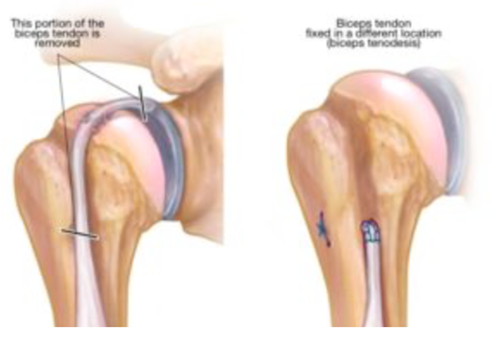
There are two tendons at the top end of the biceps muscle in the arm. The longer of these two tendons goes through the shoulder joint to attach to the top of the socket of the shoulder, and can often become inflamed where it passes through the joint. This is a common source of shoulder pain. (The shorter tendon attaches at the front of the shoulder, outside the joint, and is actually the tendon that does most of the work of the biceps.) In order to treat pain from biceps inflammation, termed tenosynovitis, the long head of the biceps can be detached from its insertion at the top of the socket of the shoulder joint. This is called a tenotomy of the biceps. It can be left to retract down out of the joint, or it can be retrieved and reattached outside the joint. Typically in younger or more active patients, the tendon is reattached, and this is a biceps tenodesis. Ms. Delaney’s method of choice for performing tenodesis is to reattach the tendon to the humerus bone underneath the pectoral muscle (pectoralis major), using a suture anchor that is placed into the bone and which allows the tendon to be stitched to bone, after the inflamed or worn part of the tendon has been removed. The tendon detachment (tenotomy) is done arthroscopically (keyhole) and then the reattachment is done via a mini-open approach using a small incision (2-3cm) just above the armpit.
Risks
There is a small risk (<1%) of damage to nerves or blood vessels, or infection. You will receive antibiotics from the anaesthetist at the beginning of surgery to minimise the risk of infection. A small percentage of patients develop stiffness of the shoulder after surgery (<5%). The reattached tendon can become detached (converting the tenodesis to a simple tenotomy) if you do not observe the post-operative restrictions. This will still allow for pain relief from the biceps inflammation or tenosynovitis, but may lead to a noticeable difference in the contour of the biceps muscle in the arm, and in some cases (approximately 15% of tenotomy cases) to cramping of the muscle. As with any surgical procedure, a small proportion of patients may fail to derive benefit from the surgery or may require further procedures.
POST-OPERATIVE CARE
Pain Control
It is normal to have swelling around the shoulder and some discomfort or pain after surgery. As the fluid used during surgery to expand the shoulder joint is gradually reabsorbed by your body, the swelling will decrease over 2-3 days after surgery. The post-operative pain should be controlled by pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day).
Sling
You will be placed in a sling at the end of your surgery in order to protect reattached biceps tendon and allow it to heal to its new location on the humerus bone. The sling is to be worn at all times, including during sleep, for a period of 3 weeks. If you have had other procedures, such as a rotator cuff repair for example, in conjunction with your biceps tenodesis, then the time in the sling may be longer. The physiotherapist will instruct you on managing with the sling while protecting your repair. Wrist and hand motion are allowed and encouraged.
Wounds
There will typically be a number of small incisions about the shoulder, covered by waterproof dressings. Leave the waterproof dressings in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. If the dressings get wet during those first 7 days, replace them with clean, dry dressings. Skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you have the correct physiotherapy instructions.
Rehabilitation
At your first post-operative visit, Ms. Delaney will give you a prescription for physiotherapy and a detailed post-operative protocol for you and your physiotherapist to follow. In general, for the first 3 weeks after surgery, all movements with the shoulder will be passive. Active movements will begin as you transition out of the sling. The focus will then be on regaining your shoulder motion gradually. No strengthening will be allowed until 6 weeks typically.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving, depending on the amount of time you have to spend in the sling.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney.
Return to Leisure Activities
Return to leisure activities or sports will depend on your progress with physiotherapy. Ms. Delaney and your physiotherapist will advise you on the timing of your return to leisure activities.
Capsular Release
Introduction
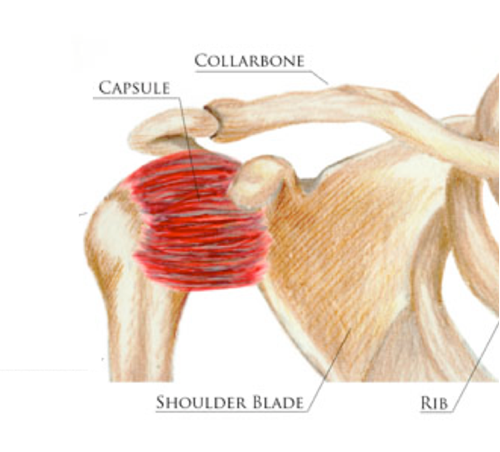
Capsular release surgery is performed when there is significant shoulder stiffness and pain due to adhesive capsulitis, or frozen shoulder. This can be primary i.e. idiopathic (with no known cause) or secondary to shoulder surgery or trauma. In either case, it is an inflammatory process in the capsular tissue and ligaments around the shoulder that causes them to become thickened and inflamed. The initial approach to treatment involves anti-inflammatory medications, corticosteroid injections, in some cases oral steroids for a very short period of time, and a gentle stretching programme. If these measures fail, then capsular release surgery may be appropriate.
Prior to your capsular release surgery, it is very important that you set up your physiotherapy appointments in advance and have them scheduled to start the day after your discharge from the hospital. You will typically stay one night in the hospital after surgery to facilitate immediate physiotherapy and shoulder motion while in hospital. Therefore, you should book your first post-operative physiotherapy appointment for day two after surgery. You will be sent home with a detailed physiotherapy prescription for you and your physiotherapist to follow. You need to attend physiotherapy 3 times the first and second weeks, then twice a week after that, depending on your progress. You will have a home exercise programme to follow daily. The success of your capsular release procedure depends in large part on your immediate post-operative rehabilitation.
Arthroscopic Capsular Release Surgery
The surgery is performed under general anaesthesia. This is an arthroscopic (“keyhole” surgery), with a number of small, 5mm incisions. The thickened, inflamed capsular tissue is divided and released, using a combination of small instruments. Inflamed tissue within the shoulder joint (synovitis) is removed. If there is severe inflammation of the biceps tendon, as is sometimes found, the tendon may also be released from within the joint (biceps tenotomy). The space above the shoulder joint and under the point of the shoulder, called the subacromial space, may also have some inflamed tissue or bursitis, and this will also be removed if present in order to maximise pain relief.
Risks
There is a very small risk (<1%) of bleeding, infection or damage to nerves. You will be given antibiotics by the anaesthetist at the beginning of surgery to minimise the risk of infection. There is a risk of recurrent shoulder stiffness, which is why post-operative rehabilitation is of key importance.
POST-OPERATIVE CARE
Pain Control
It is normal to have some swelling around the shoulder and some discomfort or pain after surgery. As the fluid used during surgery to expand the shoulder joint is gradually reabsorbed by your body, the swelling will decrease over 2-3 days after surgery. The post-operative pain should be controlled by pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day). It is important to have good pain control to allow you to participate fully in your post-operative rehabilitation. An anti-inflammatory (such as Vimovo, Difene, Nurofen or similar) is a helpful component of the pain control regimen after this procedure.
Sling
You will be placed in a basic sling at the end of your surgery. This sling is for comfort only and should be discarded as early as possible. Shoulder motion is strongly encouraged. The arm can be used normally for activities of daily living. The physiotherapist will work with you in the hospital immediately after your surgery to begin moving the shoulder in order to maximise gains in motion achieved at surgery.
Wounds
There will typically be a number of small incisions about the shoulder, covered by waterproof dressings. Leave the waterproof dressings in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. Skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you are making appropriate progress with physiotherapy.
Rehabilitation
See above. Physiotherapy will commence immediately after surgery. Once your wounds have healed at about 2 weeks post surgery, you will be strongly encouraged to do your shoulder exercises in a swimming pool, as this has been found to be very beneficial for stiff shoulder problems.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney. Physiotherapy needs to be a priority in the first two weeks after surgery and it is usually advisable to be off work for this period of time.
Return to Leisure Activities
Return to leisure activities and sports will depend on the type of sport and your rehabilitation progress. Ms. Delaney and your physiotherapist will advise you on the timing of your return to sport. Once you have regained full, comfortable shoulder range of motion, you can resume strengthening exercises for your shoulder and gradually return to leisure activities involving the shoulder.
Rotator Cuff Repair
Introduction
These are general guidelines, but each patient’s shoulder condition is unique and Ms. Delaney will discuss with you the specific details relevant to your case.
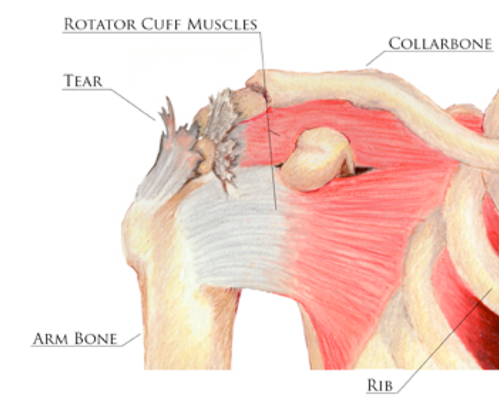
The rotator cuff is a group of four muscles whose tendons surround the shoulder joint and insert onto the humerus, or the ‘ball’ of the ball and socket joint of the shoulder. The function of the rotator cuff muscles is to help keep the ball in the socket as well as to initiate and contribute to certain shoulder movements.
Rotator Cuff Tears
The rotator cuff tendons commonly degenerate over time, which is often associated with inflammation and tendinitis. In addition, the bony prominence at the top of the shoulder, called the acromion, or the joint between this and the collarbone, may have a bony spur that can narrow the space available below them for the tendons to travel through. Eventually, with repeated minor tears or ongoing degeneration of the tendons, a full thickness tear may occur and this can often be painful. A full thickness tear may be associated with weakness or difficulty using the arm.
In some patients, full thickness rotator cuff tears can occur with a distinct traumatic episode, such as a fall. This can happen in patients whose tendons have not undergone any prior degeneration and who may be relatively young.
The options for treatment of rotator cuff tears include symptomatic management with injections and physiotherapy, as well as in some cases surgery to repair the tear. Ms. Delaney will advise you on the option most suited to your tear and your individual situation.
The chances of a successful repair are influenced by factors such as the size of the tear, the quality of the tendon tissue, and whether any muscle wasting has occurred in the muscles of the rotator cuff. In addition, smoking has been shown to negatively affect the healing of a rotator cuff repair.
Rotator Cuff Repair
Surgery to repair the rotator cuff tendons is performed under general anaesthesia and is typically done arthroscopically (“key-hole”) via small incisions of approximately 5mm length. The tendons are repaired by stitching them back down to the bony surface where they normally attach, using suture anchors inserted into the bone. The arm is kept in a sling for 4-6 weeks after surgery, depending on the size of the tear and the quality of the repair. It is important to note that rehabilitation after rotator cuff repair involves months of physiotherapy and progress is gradual. It often takes 6-12 months to derive the full benefit from the surgery.
Risks
There is a small risk (<1%) of damage to nerves or blood vessels or infection. You will receive antibiotics from the anaesthetist at the beginning of surgery to minimise the risk of infection. A small percentage of patients develop stiffness of the shoulder after surgery (<5%). Most rotator cuff tears have occurred because the tendon was degenerative and these tendons cannot be expected to heal as a normal tendon. Failure to heal or repeat tearing can occur in a minority of cases. Overall, the surgery is successful in about 80% of patients. As with any surgical procedure, a small proportion of patients may fail to derive benefit from the surgery or may require further procedures.
POST-OPERATIVE CARE
Pain Control
It is normal to have swelling around the shoulder and some discomfort or pain after surgery. As the fluid used during surgery to expand the shoulder joint is gradually reabsorbed by your body, the swelling will decrease over 2-3 days after surgery. The post-operative pain should be controlled by pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day).
Sling
You will be placed in a sling at the end of your surgery in order to protect the repair and allow the tendons to heal. The sling is to be worn at all times, including during sleep, for a period of 4 – 6 weeks, depending on the size of the tear and the quality of the tendon tissue repaired. The physiotherapist will instruct you on managing with the sling while protecting your repair. Elbow, wrist and hand motion are allowed and encouraged.
Wounds
There will typically be a number of small incisions about the shoulder, covered by waterproof dressings. Leave the waterproof dressings in place for 10 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. Skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2 weeks after surgery. Ring the office at 01-5262335 to confirm this appointment.
Rehabilitation
At your first post-operative visit, Ms. Delaney will give you a prescription for physiotherapy and a detailed post-operative protocol for you and your physiotherapist to follow. In general, for the first 6 weeks after surgery, all movements with the shoulder will be passive. Active movements will begin as your transition out of the sling. The focus will then be on regaining your shoulder motion gradually. No strengthening will be allowed until 12 weeks typically.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving, depending on the amount of time you have to spend in the sling.
Return to Work
Return to work depends on the size of the tear, the quality of the repair, and the nature of your occupation. You need to discuss this with Ms. Delaney.
Return to Leisure Activities
Return to leisure activities or sports will depend on the size of your tear, the quality of the repair, and your progress with physiotherapy. Ms. Delaney and your physiotherapist will advise you on the timing of your return to leisure activities.
Shoulder Replacement - Anatomic
Introduction
Arthritis of the shoulder joint leads to pain and limitation of motion. In arthritis, the cartilage surface of the joint has been worn away. There is often overgrowth of bone as the body attempts to heal, called osteophytes, which contribute to the altered mechanics, stiffness and pain. It is not possible for the cartilage to heal or regenerate, and the pain continues. Shoulder arthritis can be treated with conservative approaches such as injections and anti-inflammatory medications. When symptoms reach the point where the patient feels they are having a significant impact on daily life, and conservative measures are failing to relieve these symptoms adequately, then the patient may be a candidate for shoulder replacement surgery. Shoulder replacement replaces both the ball (humeral head) and the socket (glenoid) of the shoulder joint. The humeral head is replaced with a metal component after removal of the arthritic parts, and the glenoid is replaced with a plastic (polyethylene) component.
Prior to shoulder replacement surgery, Ms. Delaney will usually request a CT scan of your shoulder to see the extent of deformity of the joint and to allow for surgical planning.
These are general guidelines, but each patient’s shoulder condition is unique and Ms. Delaney will discuss with you the specific details relevant to your case.

Shoulder Replacement Surgery
The surgery is performed under general anaesthesia. The incision is in the front of the shoulder and provides access to the shoulder joint by detaching a tendon at the front of the shoulder, the subscapularis tendon. The arthritic joint surfaces are removed, and replaced with the implant components. In addition, the top portion of the biceps tendon, which is usually degenerative, inflamed and painful in association with the shoulder arthritis, is removed and the biceps is reattached further down the arm. The subscapularis is carefully repaired at the end of surgery.

Risks
Risks of shoulder replacement surgery include damage to nerves or blood vessels and infection. You will be given antibiotics by the anaesthetist at the beginning of surgery and for the following 24 hours to minimise the risk of infection. Longer term risks include instability or dislocation of the replacement, loosening of the socket, or further trauma causing fracture or loosening. Shoulder replacement surgery is successful in over 90% of patients.
POST-OPERATIVE CARE
Pain Control
It is to be expected that there will be some pain and discomfort after surgery. You will be given pain medication in hospital and you will be sent home with a prescription for pain medication. The post-operative pain should be controlled by the pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day).
Sling
You will be placed in a sling at the end of your surgery, largely to protect the subscapularis tendon repair. The physiotherapist will show you how to manage the sling while protecting the shoulder. You will commence some gentle pendulum and passive motion exercises with the shoulder early in your rehabilitation, within limits prescribed by Ms. Delaney, but the sling is to be worn at all other times, including sleep, for 4 weeks. At that point, you will transition out of the sling and begin active motion of the shoulder, under supervision of your physiotherapist and Ms. Delaney.
Wound
The wound will be covered by a waterproof dressing. Leave this dressing in place for 10 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. Skin stitches are usually absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2 weeks after surgery. Ring the office at 01-5262335 to confirm this appointment.
Rehabilitation
At your follow up visit with Ms. Delaney, you will be given a prescription for physiotherapy and a detailed physiotherapy protocol for you and your physiotherapist to follow. Typically, you will spend 4 weeks in a sling, during which time you will be allowed to do some supervised, passive motion exercises, followed by active motion exercises after the 4-week point, with any strengthening usually deferred until 12 weeks.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney. If you work in a job that involves heavy impact loading of the shoulder, this puts the joint replacement at risk for loosening and failure, and this needs to be discussed prior to your surgery.
Return to Leisure Activities
You will be advised on return to sports and leisure activities by Ms. Delaney and your physiotherapist. In the long term, patients generally can participate in most of their desired sports, with the exception of collision and contact activities. Skiing is permissible, but falling risks fracture of the shoulder and loosening of the prosthesis.
Antibiotic Prophylaxis
After joint replacement, it is important that you take a preventative antibiotic prior to any dental work, as even a simple dental cleaning can cause bacteria to enter your bloodstream and infect your shoulder replacement. Ms. Delaney can provide you with a prescription for this antibiotic whenever you need it – please call the office.
Shoulder Replacement - Reverse
Introduction
Arthritis of the shoulder joint leads to pain and limitation of motion. In arthritis, the cartilage surface of the joint has been worn away. There is often overgrowth of bone as the body attempts to heal, called osteophytes, which contribute to the altered mechanics, stiffness and pain. It is not possible for the cartilage to heal or regenerate, and the pain continues. Shoulder arthritis can be treated with conservative approaches such as injections and anti-inflammatory medications. When symptoms reach the point where the patient feels they are having a significant impact on daily life, and conservative measures are failing to relieve these symptoms adequately, then the patient may be a candidate for shoulder replacement surgery. When there is also a large tear of the rotator cuff tendons, or in certain other situations when there is a significant amount of bony loss associated with the arthritis, a type of shoulder replacement in which the ball and socket are reversed, may be necessary. This is a reverse shoulder replacement.
Prior to shoulder replacement surgery, Ms. Delaney will usually request a CT scan of your shoulder to see the extent of deformity of the joint and to facilitate surgical planning on a dedicated software programme that allows an individual, 3D plan to be generated for your shoulder.
This leaflet provides general guidelines, but each patient’s shoulder condition is unique and Ms. Delaney will discuss with you the specific details relevant to your case.

Reverse Shoulder Replacement Surgery
The surgery is performed under general anaesthesia. The incision is in the front of the shoulder. The arthritic joint surfaces are removed, and replaced with the implant components. In addition, the top portion of the biceps tendon, which is usually degenerative, inflamed and painful in association with the shoulder arthritis, is removed and the biceps is reattached further down the arm.
Risks
Risks of reverse shoulder replacement surgery include damage to nerves or blood vessels and infection. You will be given antibiotics by the anaesthetist at the beginning of surgery and for the following 24 hours to minimise the risk of infection. Longer term risks include failure of the prosthesis, instability or dislocation of the replacement, or further trauma causing fracture or loosening. The overall rate of complications is lower for patients who have not had a prior shoulder replacement (10%), when compared to patients undergoing a reverse shoulder replacement as a revision surgery (20%). Patient satisfaction rates with reverse shoulder replacement surgery are generally above 90%.
POST-OPERATIVE CARE
Pain Control
It is to be expected that there will be some pain and discomfort after surgery. You will be given pain medication in hospital and you will be sent home with a prescription for pain medication. The post-operative pain should be controlled by the pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day).
Sling
You will be placed in a sling at the end of your surgery. The physiotherapist will show you how to manage the sling while protecting the shoulder. The sling is to be worn at all times, including sleep, for 4 weeks. At 4 weeks, you will transition out of the sling and begin active motion of the shoulder, under supervision of your physiotherapist and Ms. Delaney.
Wound
The wound will be covered by a waterproof dressing. Leave the waterproof dressing in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. If the dressing gets wet during those first 7 days, replace it with a clean, dry dressing. All skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. You will also have an X-ray that day. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you have the correct physiotherapy instructions.
Rehabilitation
At your follow up visit with Ms. Delaney, you will be given a prescription for physiotherapy and a detailed physiotherapy protocol for you and your physiotherapist to follow. Typically, you will spend 4 weeks in a sling, during which time you may be allowed to do some supervised, passive motion exercises, followed by active motion exercises after the 4-week point, with any strengthening usually deferred until 12 weeks. Your physiotherapist will demonstrate to you the precautions in terms of position and movements to avoid dislocation of the prosthesis.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney. If you work in a job that involves heavy impact loading of the shoulder, this puts the joint replacement at risk for loosening and failure, and this needs to be discussed prior to your surgery.
Return to Leisure Activities
You will be advised on return to sports and leisure activities by Ms. Delaney and your physiotherapist. In the long term, it is recommended to notuse the operative arm for high demand activities such as heavy lifting, carpentry, chopping wood, or contact and collision sports. Ms. Delaney generally recommends that patients should not perform strenuous activities with their arm, to prevent early failure of the reverse prosthesis due to overuse. Obeying activity restrictions ensures increased longevity of the reverse prosthesis. Activities such as golf, however, seem to be well tolerated.
Antibiotic Prophylaxis
After joint replacement, it is important that you take a preventative antibiotic prior to any dental work, as even a simple dental cleaning can cause bacteria to enter your bloodstream and infect your shoulder replacement. Ms. Delaney can provide you with a prescription for this antibiotic whenever you need it – please call the office.
Shoulder Stabilisation Surgery - Bankart Procedure
Introduction
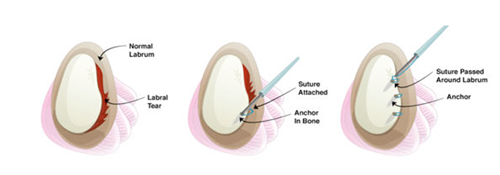
The shoulder is a very mobile joint but is therefore susceptible to instability. Instability occurs when the ‘ball’ (the head of the humerus bone) comes out, or partially comes out of the ‘socket’ (the glenoid). The socket is shallow and has a cartilage ‘bumper’ around its circumference called the labrum, which helps deepen the socket and increase stability. The capsule of the shoulder joint is made up of strong ligaments, which blend with the labrum and contribute to shoulder stability. When a dislocation or subluxation (partial dislocation) event occurs, the labrum and/or the ligaments tear. The term Bankart lesion is used to describe the labral tear. This is common in contact sports or with repeated overhead activities, but can occur with any trauma. It is far more common for the direction of instability, and therefore the labral tear, to be anterior or in the front of the shoulder, but in some cases the instability and labral tear may be at the back of the shoulder (posterior) – in these cases similar guidelines apply in terms of surgery and rehabilitation.
Each patient’s shoulder is unique, and Ms. Delaney will discuss the details of your individual situation with you. The following are some general guidelines.
Labral Repair Surgery (Bankart procedure)
The surgery is performed under general anaesthesia. It is often performed arthroscopically (“keyhole”) via a number of small, 5mm incisions. In certain circumstances the repair may be done as an open procedure through an incision in the front of the shoulder. Ms. Delaney will discuss this with you and will decide based on the severity of the labrum injury, your age, and the sports you play, which procedure is best for you. Certain patients may need a different type of open stabilisation procedure, a Latarjet procedure, when there is damage to the bone of the socket. Ms. Delaney will discuss this with you if it is relevant to your individual situation. Sometimes, this decision is made at surgery when Ms. Delaney examines the shoulder under anaesthesia and with an arthroscope (camera) in the joint.
In a Bankart repair, the labrum is repaired by stitching it back to the bone of the socket, using suture anchors placed in the bone.
Risks
There is a small risk (<1%) of damage to nerves or blood vessels, infection, or stiffness. You will receive antibiotics from the anaesthetist at the beginning of surgery to minimise the risk of infection. This surgery is successful in 90% of patients. Further trauma to the shoulder can lead to recurrence of instability in a small number of patients and may require further surgery.
POST-OPERATIVE CARE
Pain Control
The shoulder will usually be sore and painful immediately after surgery. You will be sent home from the hospital with prescription pain medication. The post-operative pain should be controlled by pain medicine and ice. Apply ice, in the form of ice packs or crushed ice/frozen peas wrapped in a damp cloth, to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day). Avoid anti-inflammatory medication (Neurofen, Difene etc) for the first 30 days after surgery.
Sling
You will be placed in a shoulder immobiliser sling at the end of your surgery in order to protect the repair. The sling is to be worn at all times, including during sleep, for a period of 4 weeks. The physiotherapist will instruct you on managing with the sling while protecting your repair. Elbow, wrist and hand motion are allowed and encouraged.
Wounds
After the arthroscopic procedure, there will typically be a number of small incisions about the shoulder, covered by waterproof dressings. An open procedure will have an additional, larger incision in the front of the shoulder. Leave the waterproof dressings in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. If the dressings get wet during those first 7 days, replace them with clean, dry dressings. All skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you have the correct physiotherapy instructions.
Rehabilitation
At your first post-operative visit, Ms. Delaney will give you a prescription for physiotherapy and a detailed post-operative protocol for you and your physiotherapist to follow. At 2 weeks, you may resume cardio training on an exercise bike if desired. In general, for the first 4 weeks after surgery, all movements with the shoulder will be passive. Active movements will begin as you transition out of the sling. The initial focus will then be on regaining your shoulder motion, while maintaining shoulder stability.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney.
Return to Sports
Return to sports will depend on the type of sport and your progress with physiotherapy. Ms. Delaney and your physiotherapist will advise you on the timing of your return to sport. The labrum typically takes 12-16 weeks to heal. Return to sport is dependent on that and on regaining good range of motion, strength and scapular stability. In general, contact athletes return to full contact at about 6 months post-operatively.
Shoulder Stabilisation Surgery - Latarjet Procedure
Introduction
The shoulder is a very mobile joint but is therefore susceptible to instability. Instability occurs when the ‘ball’ (the head of the humerus bone) comes out, or partially comes out of the ‘socket’ (the glenoid). The socket is shallow and has a cartilage ‘bumper’ around its circumference called the labrum, which helps deepen the socket and increase stability. The capsule of the shoulder joint is made up of strong ligaments, which blend with the labrum and contribute to shoulder stability. When a dislocation or subluxation (partial dislocation) event occurs, the labrum and/or the ligaments tear. In association with this injury, especially with repeated dislocations or subluxations, the bone at the rim of the socket may sustain damage, as well as the bone at the back of the ‘ball’ or humerus.
Each patient’s shoulder is unique, and Ms. Delaney will discuss the details of your individual situation with you. The following are some general guidelines.
Latarjet Procedure
The surgery is performed under general anaesthesia. This is performed as an open surgery, through an incision in the front of the shoulder. In some cases, the decision to perform this surgery rather than a soft tissue repair (Bankart or labrum repair) is made at surgery when Ms. Delaney examines the shoulder under anaesthesia and with an arthroscope (camera) in the joint, therefore it is common to undergo a diagnostic arthroscopy (“keyhole” surgery) at the beginning of the procedure. This is a more accurate method than MRI or CT scan of assessing the injury to the structures of the shoulder.
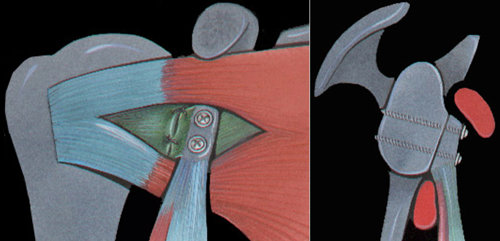
Images courtesy G. Walch
In the Latarjet procedure, a piece of bone is taken from part of the front of the shoulder blade or scapula called the coracoid, and transferred to the front of the
socket of the shoulder, the glenoid. It is passed through a split in a tendon at the front of the shoulder for added stability, before being secured to the front of the glenoid, typically with two screws.
Risks
There is a small risk (approximately 1%) of damage to nerves or blood vessels, or infection. You will receive antibiotics from the anaesthetist at the beginning of surgery to minimise the risk of infection. There is a risk (approximately 5%) of temporary nerve damage related to stretch of the nerves around the shoulder with this procedure. If this occurs, it most commonly involves just a small patch of numbess but in some cases there can be minor weakness also. This typically resolves over a number of weeks without any intervention. Occasionally, the screws used to fix the bone graft to the socket may need to be removed once the bone graft has healed, in order to relieve any nerve irritation. Stiffness can occur but is rare with adherence to the rehabilitation protocol. This surgery is successful in 90-95% of patients. Further trauma to the shoulder can lead to recurrence of instability in a small number of patients and may require further surgery.
POST-OPERATIVE CARE
Pain Control
The shoulder will usually be sore and painful immediately after surgery. You will be sent home from the hospital with prescription pain medication. The post-operative pain should be controlled by pain medicine and ice. Apply ice to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day). Avoid anti-inflammatory medication (Neurofen, Difene etc) for the first 30 days after surgery.
Sling
You will be placed in a sling or shoulder immobliser at the end of your surgery. The sling is to be worn at all times, including during sleep, for a period of 3 weeks. The physiotherapist will instruct you on managing with the sling while protecting your repair. Elbow, wrist and hand motion are allowed and encouraged.
Wounds
Your incisions will be covered by waterproof dressings. Leave the waterproof dressings in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. If the dressings get wet during those first 7 days, replace them with clean, dry dressings. All skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you have the correct physiotherapy instructions.
Rehabilitation
At your first post-operative visit, Ms. Delaney will give you a prescription for physiotherapy and a detailed post-operative protocol for you and your physiotherapist to follow. At 2 weeks, you may resume cardio training on an exercise bike if desired. In general, for the first 2 weeks after surgery, all movements with the shoulder will be passive. Active movements will begin as you transition out of the sling. The initial focus will then be on regaining your shoulder motion, while maintaining shoulder stability.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney.
Return to Sports
Return to sports will depend on the type of sport and your progress with physiotherapy. Ms. Delaney and your physiotherapist will advise you on the timing of your return to sport. The transferred bone graft typically takes 12 weeks to completely heal. Return to sport is dependent on that and on regaining good range of motion, strength and scapular stability. In general, contact athletes return to full contact at about 3-4 months post-operatively.
Subacromial Decompression
Introduction
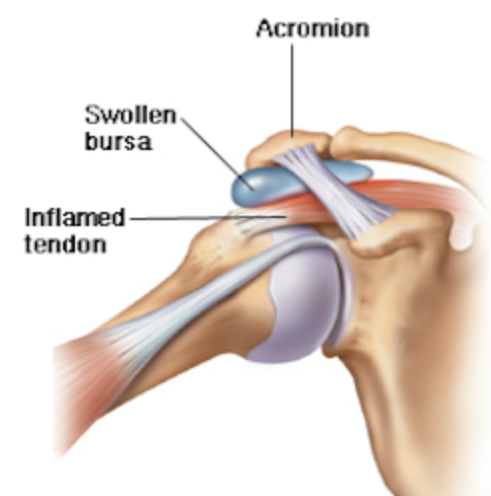
The subacromial space is an area above the main shoulder joint, through with the tendons of the rotator cuff pass. These tendons can often become inflamed and swollen, causing pain. The tissue around the tendons, called bursa, also becomes inflamed, termed bursitis. In addition, the so-called ‘point of the shoulder’, or the acromion, which is a projection of bone from the shoulder blade, can be shaped in such a way as to further limit the space for the tendons to travel through. The acromion makes a joint with the outer end of the clavicle, which can be another source of pain.
Subacromial decompression surgery
The surgery is performed under general anaesthesia. This is an arthroscopic (“keyhole” surgery), with a number of small, 5mm incisions. The inflamed bursal tissue around the tendons is cleared away with a combination of small, arthroscopic instruments, and any bony prominence is smoothed down using a shaver or burr. If the joint between the acromion and the collarbone (the AC or acromioclavicular joint) has been painful on clinical exam in the office and is found to be contributing to any bony prominence seen at arthroscopy, then it too is smoothened with the burr, and any arthritic bone ends of the AC joint are removed.
Risks
There is a very small risk (<1%) of bleeding, infection, damage to nerves, or shoulder stiffness. You will be given antibiotics by the anaesthetist at the beginning of surgery to minimise the risk of infection.
POST-OPERATIVE CARE
Pain Control
It is normal to have some swelling around the shoulder and some discomfort or pain after surgery. As the fluid used during surgery to expand the shoulder joint is gradually reabsorbed by your body, the swelling will decrease over 2-3 days after surgery. The post-operative pain should be controlled by pain medicine and ice. Apply ice, in the form of ice packs or crushed ice/frozen peas wrapped in a damp cloth, to the shoulder frequently (approximately 20 mins at a time, at least 2-3 times a day).
Sling
You will be placed in a basic sling at the end of your surgery. This sling is for comfort only and can start to be removed in the initial days after surgery. Shoulder motion is encouraged. The arm can be used normally for activities of daily living.
Wounds
There will typically be a number of small incisions about the shoulder, covered by waterproof dressings. Leave the waterproof dressings in place for 7 days to allow wound healing. You may shower 72 hours (3 days) after surgery, but do not soak the shoulder in the bath or go into a pool until after cleared to do so at your follow up appointment with Ms. Delaney. If the dressings get wet during those first 7 days, replace them with clean, dry dressings. Skin stitches are absorbable and do not need to be removed.
Follow up Appointments
An appointment will be made for you to see Ms. Delaney approximately 2-3 weeks after surgery and you will be informed by text message. If you need to reschedule your assigned post-operative appointment, please ring 01-5262335. It is important that you are seen for your post-operative visit around the 2-3 week post-op time frame in order to check your wound healing and ensure that you have the correct physiotherapy instructions.
Rehabilitation
Many patients after subacromial decompression surgery progress quite quickly on their own and need minimal, if any, supervised physiotherapy. At your first post-operative visit, Ms. Delaney will give you a prescription for physiotherapy, if needed, and a detailed post-operative protocol for you and your physiotherapist to follow.
Driving
You must not drive while in the sling or while taking narcotic pain medication. Ms. Delaney will advise when you may begin driving.
Return to Work
Return to work depends on the nature of your occupation. You need to discuss this with Ms. Delaney. After subacromial decompression, most patients return to work within about a week.
Return to Leisure Activities
Return to leisure activities and sports will depend on the type of sport and your rehabilitation progress. Ms. Delaney and your physiotherapist will advise you on the timing of your return to sport. Once you have regained full, comfortable shoulder range of motion, you can resume strengthening exercises for your shoulder and gradually return to leisure activities involving the shoulder.
MS. DELANEY EXPLAINS SOME ASPECTS OF SHOULDER SURGERY IN THE FOLLOWING VIDEOS.
Shoulder Surgery: what to expect
Rotator Cuff Repair
Post-operative Shoulder Immobiliser
After some shoulder surgeries (rotator cuff repair, instability surgery and shoulder replacements), more support is required than a simple sling and we therefore use a shoulder immobiliser with a cushion. This video demonstrates how to wear your shoulder immobiliser and how to take it on and off.
ADDITIONAL RESOURCES:
Ms. Delaney trained at the Boston Shoulder Institute with JP Warner, Harvard professor of orthopaedic surgery and Chief of the Shoulder Service at Massachusetts General Hospital. She has contributed to that website's content and the information there is consistent with Ms. Delaney's approach to shoulder surgery. To find information on your shoulder condition or surgery, go to Patient Modules and select the appropriate section from the drop-down menu.
The American Academy of Orthopaedic Surgeons' resource for patients.